Policy
The NCDI Poverty Network supports health leaders as they develop policies that prioritize equitable, cost-effective health interventions.
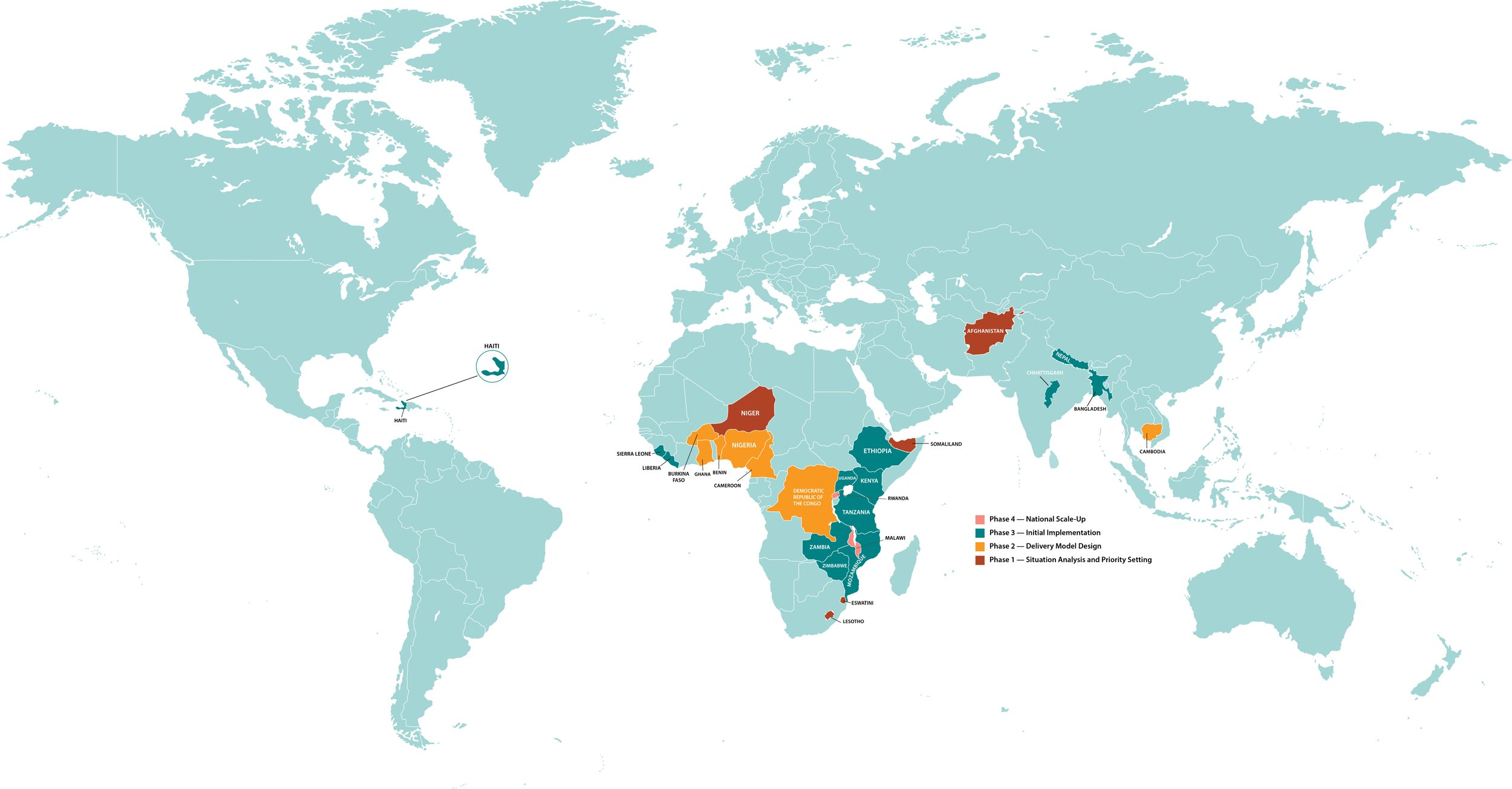
National NCDI Poverty Commissions—which are composed of Ministry of Health policymakers, clinicians, academic researchers, health planning and financing experts, implementing partners and donors, and people living with severe conditions—are the backbone of the NCDI Poverty Network.
The Network’s Policy Team works with National Commissions to develop policies that prioritize equitable, cost-effective interventions to address severe conditions disproportionately affecting children and young adults living in extreme poverty. In particular, the Policy Team supports National Commissions in countries that have recently joined the Network in working through the first phase of the Network’s Four-Phase Theory of Change: Situation Analysis and Priority-Setting.
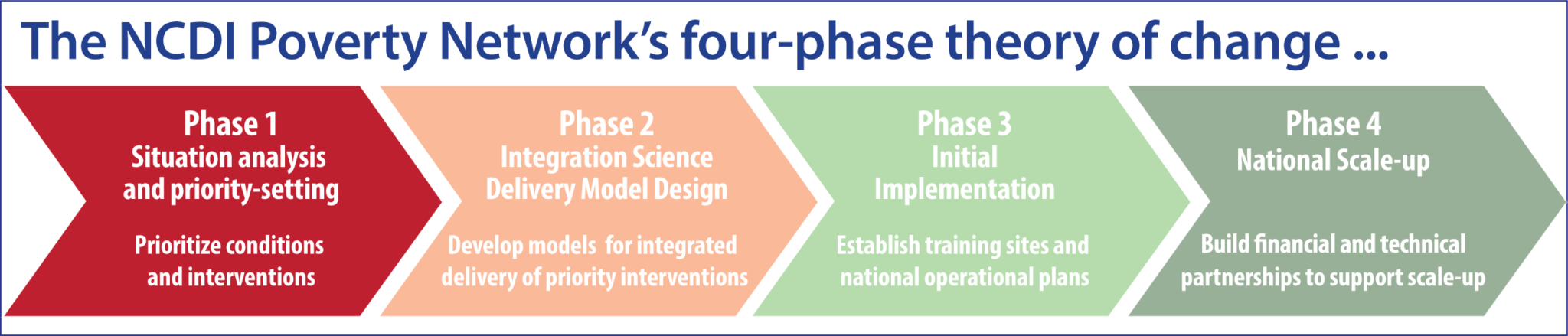
During this first phase of the Network process, National Commissions analyze the national burden of NCDs and injuries, disaggregated by age, sex, and socioeconomic status, and assess the availability and coverage of NCDI services at different levels of the health system, in order to understand disparities in prevalence, access to services, and outcomes for poor and marginalized populations. Based on findings from this situation analysis, Commissions then prioritize conditions and interventions to address the burden, taking into account both cost-effectiveness and equity, and estimate the cost and potential impact of prioritized interventions as well as the fiscal space required to implement them. Finally, Commission members disseminate their key findings and recommendations to elevate equitable access to care and treatment for severe conditions that disproportionately impact the poorest children and young adults as a priority for national policies and financing.
The Policy Team supports countries through this process by:
Sharing analytical frameworks, methods, and tools developed by the Lancet NCDI Poverty Commission, as well as a priority-setting tool developed in collaboration with the Center for Integration Science in Global Health Equity research team and the Bergen Center for Ethics in Priority-Setting;
Facilitating exchanges of experience and lessons learned with more than a dozen countries that have successfully completed this phase; and
Assisting with preparation and dissemination of reports summarizing their key findings and recommendations.
The Network’s Policy Team
-

Dr. Neil Gupta
SENIOR DIRECTOR OF POLICY
-

Christa Cepuch
MEDICINES AND HEALTH TECHNOLOGIES ADVISOR
Policy and National Commission Updates